Back in the day, someone with great insight said: ‘Most bones are filled with marrow. The tibia is filled with black ingratitude’.
Published online 2017 May 16. doi: 10.1080/17453674.2017.1321351
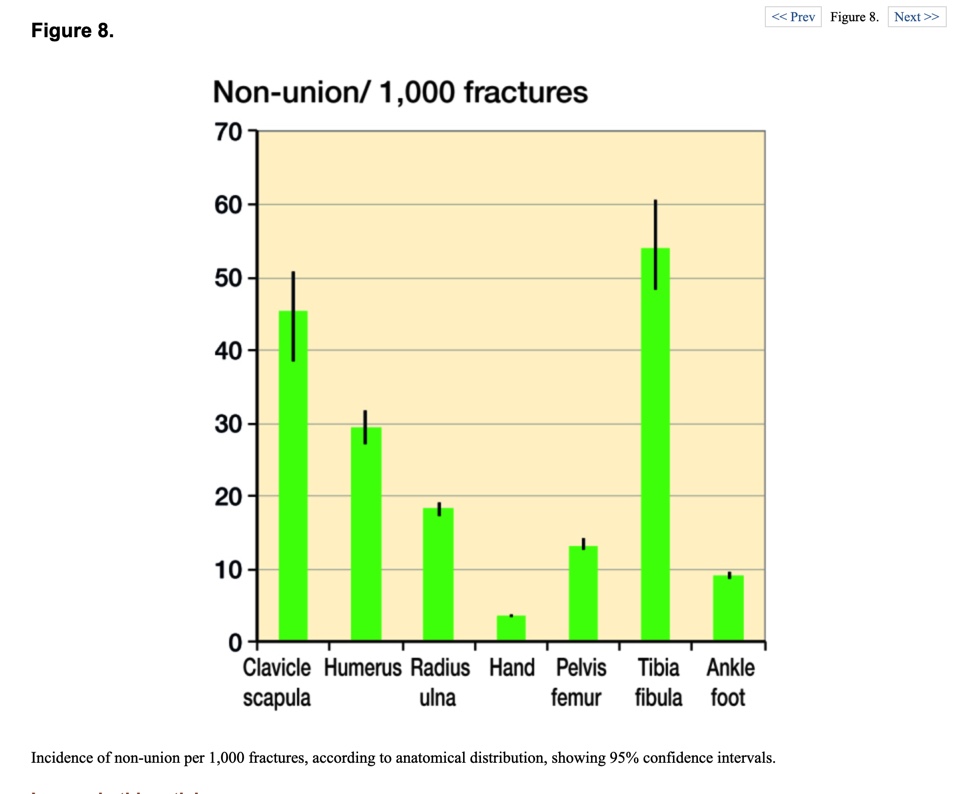
The graph above from Mills, Aitken & Simpson’s must-read paper shows the tibia to have the highest rate of non-union, followed by the clavicle. (Strictly speaking clavicle & scapula, but scapula fractures are rare and nonunions even more so, so that figure is mostly clavicular nonunion).
The tibia and clavicle have some features in common: subcutaneous through most of their length, and sparse muscle attachments to their other surfaces compared to other bones.
Just how bad is a tibial nonunion? If you look at quality of life measures, it is equivalent to end-stage hip arthrosis:
Brinker et al, ‘The Devastating Effects of Tibial Nonunion on Health-Related Quality of Life’. J Bone Joint Surg Am. 2013;95:2170-6 http://dx.doi.org/10.2106/JBJS.L.008032013
n=243, Assessment with Short Form (SF)-12 Physical Component averaged 27.4, indicating an extremely disabling effect on physical health. The AAOS Lower Limb Core Scale score averaged 52.0, consistent with high levels of physical disability. The SF-12 Mental Component averaged 42.3, indicating a substantial detrimental effect on mental health.
The factors associated with non-union (NU) in the tibia can be divided into injury-specific and person-specific.
Injury-specific factors leading to non-union
Fong et al, 2013, looked at injury-specific predictors of nonunion in 200 tibial fractures. They identified fractures with less than 25% cortical continuity as being the group with the highest probability of nonunion (I presume they meant contact, rather than continuity, as a fracture implies discontinuity). They also found that a combination of an open fracture & a fracture gap post-fixation suggested a high risk of NU.
Fong et al. ‘Predictors of nonunion and reoperation in patients with fractures of the tibia: an observational study’. BMC Musculoskeletal Disorders 2013, 14:103
http://www.biomedcentral.com/1471-2474/14/103
As well as fracture gap and open fracture, other authors have identified segmental fracture & extreme comminution as being important injury characteristics predicting NU.
Bonnevialle et al, 2003, found the following:
- 8/27 patients with segmental tibia fractures stabilized with Grosse-Kempf nail developed NU
- 2/7 external fixations developed NU
- 2/8 nailings without reaming developed NU
- Bone healing was not simultaneous in the two foci in more than half of patients.
- The 12 cases of aseptic nonunion were successfully treated by nailing with reaming and early weight bearing
Bonnevialle et al, ‘Segmental tibia fractures: a critical retrospective analysis of 49 cases’.Revue de Chirurgie Orthopedique et Reparatrice de L’appareil Moteur, 01 Sep 2003, 89(5):423-432 Language:fre
PMID: 13679742
Tilkeridis et al,’The Ilizarov method for the treatment of segmental tibial fractures’. Injury Extra, Volume 40, Issue 10, October 2009, Page 228. These authors experienced 3/33 NU.
Milenkovic, Mitkovic & Mitkovic, ‘External fixation of segmental tibial shaft fractures’, European Journal of Trauma and Emergency Surgery volume 46, pages1123–1127(2020). These authors experienced 6/32 NU (18.75%).
Severe soft tissue complications are associated with NU. (Gaston et al, 1999, ‘Fractures of the tibia – can their outcome be predicted?’J Bone Joint Surg [Br] 1999;81-B:71-6).
Compartment Syndrome (CS) is associated with a 55% incidence of delayed or nonunion, versus 17.8% in fractures without CS. (Reverte et al, ‘What is the effect of compartment syndrome and fasciotomies on fracture healing in tibial fractures?’ Injury. Volume 42, Issue 12, December 2011, Pages 1402-1407).
Arterial injury is also associated with tibial NU.
29 patients with a tibial fracture and associated vascular injury were reviewed. Fractures with an injury to the posterior tibial artery had a significantly higher nonunion rate and a greater number of weeks to union than fractures without this vascular injury. 6 ended with amputation.(Brinker, Bailey, Daniel. ‘Fracture Healing in Tibia Fractures with an Associated Vascular Injury’. The Journal of Trauma: Injury, Infection, and Critical Care: January 1997 – Volume 42 – Issue 1 – p 11-19).
Person-specific factors leading to non-union
Gaston & Simpson, ‘Inhibition of fracture healing ‘, JBJS-Br Volume 89-B, Issue 12, December 1, 2007, Pages 1553-1560.
These authors noted that gender was not a factor predisposing to NU, but that there was evidence in their review to suggest that increasing age does increase the incidence of NU.
They noted studies showing a significantly higher incidence of delayed union, nonunion, and a doubling of the time to healing of the fracture in diabetic patients.
Nutritional factors (Vitamin B6, Vitamin C, iron, calcium, phosphorus, and protein levels are all important in bone healing; deficiencies have an adverse effect on healing time and callus strength.
Alcohol has an adverse effect on bone healing, causing osteopaenia and NU.
Anti-coagulants have an effect on bone healing in animal studies, but whether this translates to clinical medicine is moot. Quite obviously there are other factors involved, and these drugs are difficult to avoid.
Antibiotics, particularly fluouroquinolones, tetracyclines, and aminoglcosides may have adverse effects on healing. In clinical practice, this concern is likely to be over-ridden in the context of sepsis, though if long-term prescription can be avoided, so much the better.
Hypothyroidism impairs endochondral ossification, with predictable effects on healing.
These authors showed that steroids also had a deleterious effect on healing, but of course decisions to stop these drugs should not be made without discussion with the prescriber for fear of precipitating a condition just as bad or worse than NU.
Non-steroidal anti-inflammatory drugs inhibit ectopic ossification around acetabular fractures. It comes as no surprise that long bone fractures having this treatment have a higher rate of NU than when ectopic ossification is prevented by DXT, or in those who had no treatment. (Burd TA, Hughes MS, Anglen JO. Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion. J Bone Joint Surg [Br] 2003;85-B:700–5).
Opiate use is also associated with NU. There is a suggestion that short-term use of painkillers is less likely to cause the problem.
Buchheit et al, ‘Opioid exposure is associated with nonunion risk in a traumatically injured population: An inception cohort study’. Injury
Volume 49, Issue 7, July 2018, Pages 1266-1271.
Smoking impairs healing of the tibia, leading to a higher rate of delayed and non-union in smokers, although non-union rates have been determined to be higher in smokers in all major lower limb bones (Patel, 2013; Santolini, 2015; Kim, 2015; Lee, 2013, Sloan, 2010, Hernigou, 2013).
In addition to the bone effects, smoking impairs soft tissue & flap healing through similar mechanisms (Morris, Marlborough, Montgomery, Allison, & Eardley. ‘Smoking and the patient with a complex lower limb injury’. Injury, 2021).